La luxación rotuliana se produce cuando la rótula abandona la articulación femoropatelar y se desplaza hacia la cara externa de la rodilla de modo que hay una pérdida de contacto total entre la rótula y la cara anterior del fémur (tróclea).
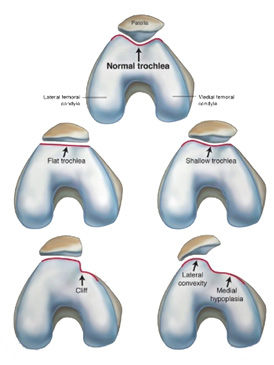

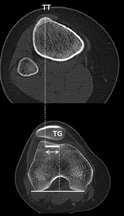
Las personas que tienen riesgo de sufrir luxación rotuliana, se caracterizan por tener alteraciones en la estructura anatómica de la rodilla como anomalías en la cara anterior del fémur (displasia troclear), rótula excesivamente alta o desplazamiento de la inserción del tendón rotuliano (distancia tuberosidad tibial anterior- garganta troclear excesiva).
Generalmente la luxación rotuliana se produce por una torsión violenta de la rodilla con un desplazamiento lateral de la rótula. Esto resulta muy invalidante para el enfermo y se acompaña de una inflamación importante por acumulación de sangre en la rodilla (hemartrosis).
La luxación rotuliana suele producirse em la segunda década de la vida, produciendo daños en el cartílago tanto de la rótula, como de la vertiente externa de la tróclea, que puede resultar irreversibles y condicionar el futuro de la rodilla.

En la actualidad no se suele intervenir la primera luxación, sino que. se trata ortopédicamente, con un periodo de movilización con la rodilla en extensión, entrono a las tres semanas.
Comienza a extenderse la opinión de intervenir incluso en la luxación rotuliana, cuando el enfermo tiene una luxación de rótula objetiva, es decir, los parámetros como profundidad de la tróclea, altura de la rótula y distancia TAGT, están significativamente alejados de la normalidad.
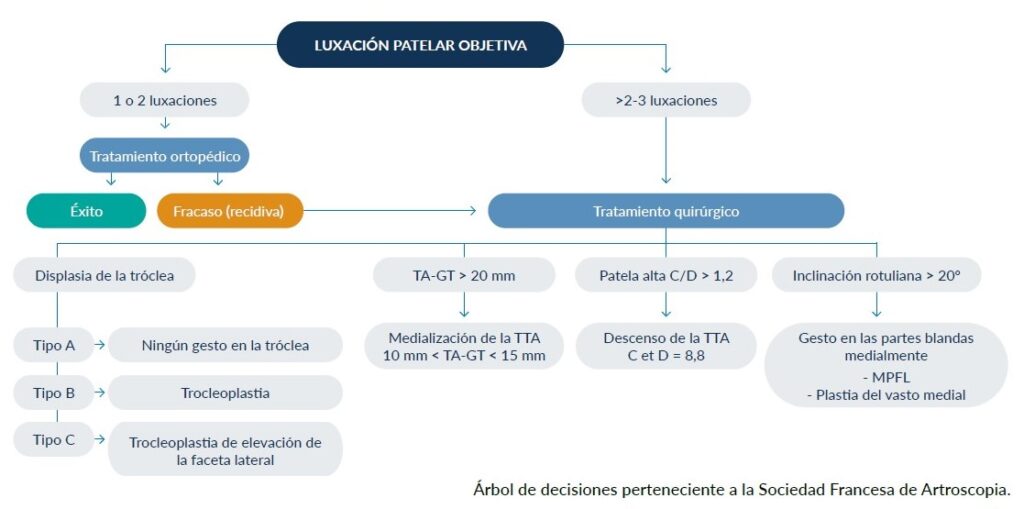
En la actualidad, practicamos una cirugía a la carta corrigiendo aquellas alteraciones de la estructura de la rodilla que están específicamente alteradas en cada paciente. Para ello, debe realizarse un estudio radiológico con TAC que determine sobre qué estructuras hemos de actuar.
En la actualidad, no es posible reproducir de forma exacta la estructura del cartílago hialino original que existía antes de la lesión. Sin embargo, disponemos de técnicas que reproducen cada vez con mayor fidelidad tejidos parecidos al hialino original, y que podríamos clasificar en tres técnicas diferentes:
Los estudios médicos indican que cuando está indicado reconstruir este ligamento, hacerlo mediante la utilización de un tendón de un donante da mejores resultados que los que obtenemos mediante la sutura.
La corrección mediante osteotomía de la tuberosidad tibial anterior mejora los resultados de la estabilización de la rótula. Es un gesto complementario de la reconstrucción del ligamento patelofemoral medial, cuando la distancia entre la tuberosidad tibial y el surco troclear sobrepasa los 20 mm (TAGT).
En términos generales y según la cirugía realizada, el paciente debe permanecer protegido con una férula de inmovilización en extensión que le permita la carga con bastones a partir de las primeras 48 horas.
Así mismo, iniciaremos movilización pasiva inmediata y progresiva a partir de las dos horas de la intervención


Una vez producida la luxación rotuliana, disponemos (tras realizar un escáner del paciente) de mediciones objetivas que nos permitirán realizar a la carta una cirugía que corrija el factor responsable de la luxación de forma precisa.
En la actualidad hemos de comprobar también mediante el sistema Go5D el comportamiento de la rótula al deslizarse por la articulación que comparte con el fémur de forma dinámica, es decir, con el paciente en movimiento y realizando aquellos movimientos que pueden poner de manifiesto una luxación de rótula lo suficientemente importante como para provocar una luxación.
La conjunción de los datos proporcionados por el TAC y por el sistema Go5D, constituirán un modelo basado en la estadística para la predicción del riesgo de que la luxación pueda volver a repetirse a medio y largo plazo después de la primera luxación. Estos datos, junto con la situación clínica del paciente, serán elementos muy valiosos para la indicación quirúrgica.
Si el enfermo no reúne los criterios objetivos que aporta el TAC ni los parámetros objetivos que aporta el examen biomecánico Go5D, debemos orientar el tratamiento hacia una actitud conservadora.
1. N. Maffulli, K. M. Chan, R. C. Bundoc, and J. C. Y. Cheng, "Knee arthroscopy in Chinese children and adolescents: an eight-year prospective study," Arthrosc. J. Arthrosc. Relat. Surg., vol. 13, no. 1, pp. 18-23, 1997.
2. F. Oliva, M. Ronga, U. G. Longo, V. Testa, G. Capasso, and N. Maffulli, "The 3-in-1 procedure for recurrent dislocation of the patella in skeletally immature children and adolescents.," Am. J. Sports Med., vol. 37, no. 9, pp. 1814-20, Sep. 2009.
3. N. Maffulli, R. C. Bundoc, K. M. Chan, and J. C. Cheng, "Paediatric sports injuries in Hong Kong: a seven-year survey.," Br. J. Sports Med., vol. 30, no. 3, pp. 218-221, 1996.
4. A. C. Bitar, M. K. Demange, C. O. D'Elia, and G. L. Camanho, "Traumatic Patellar Dislocation Nonoperative Treatment Compared with MPFL Reconstruction Using Patellar Tendon," Am. J. Sports Med., vol. 40, no. 1, pp. 114-122, 2012.
5. J. J. Stefancin and R. D. Parker, "First-time traumatic patellar dislocation: a systematic review," Clin. Orthop. Relat. Res., vol. 455, pp. 93-101, 2007.
6. S. Palmu, P. E. Kallio, S. T. Donell, I. Helenius, and Y. Nietosvaara, "Acute patellar dislocation in children and adolescents: a randomized clinical trial," J. Bone Jt. Surg., vol. 90, no. 3, pp. 463-470, 2008.
7. A. C. Colvin and R. V West, "Patellar instability," J. Bone Jt. Surg., vol. 90, no. 12, pp. 2751-2762, 2008. 8. C. Tardieu and J.-Y. Dupont, "Origine des dysplasies de la trochlée fémorale," 2008.
9. H. Dejour, G. Walch, L. Nove-Josserand, and C. H. Guier, "Factors of patellar instability: an anatomic radiographic study," Knee Surgery, Sport. Traumatol. Arthrosc., vol. 2, no. 1, pp. 19-26, 1994.
10. J. A. Feller, A. A. Amis, J. T. Andrish, E. A. Arendt, P. J. Erasmus, and C. M. Powers, "Surgical biomechanics of the patellofemoral joint," Arthrosc. J. Arthrosc. Relat. Surg., vol. 23, no. 5, pp. 542-565, 2007.
11. D. Dejour and B. Le Coultre, "Osteotomies in patello-femoral instabilities," Sports Med. Arthrosc., vol. 15, no. 1, pp. 39-46, 2007.
12. R. Y. Hinton and K. M. Sharma, "Acute and recurrentpatellar instability in the young athlete," Orthop. Clin. North Am., vol. 34, no. 3, pp. 385-396, 2003.
13. S. Ostermeier, C. Stukenborg-Colsman, C. Hurschler, and C.-J. Wirth, "In vitro investigation of the effect of medial patellofemoral ligament reconstruction and medial tibial tuberosity transfer on lateral patellar stability," Arthrosc. J. Arthrosc. Relat. Surg., vol. 22, no. 3, pp. 308-319, 2006.
14. P. J. Sillanpää, E. Peltola, V. M. Mattila, M. Kiuru, T. Visuri, and H. Pihlajamäki, "Femoral Avulsion of the Medial Patellofemoral Ligament After Primary Traumatic Patellar Dislocation Predicts Subsequent Instability in Men A Mean 7-Year Nonoperative Follow-Up Study," Am. J. Sports Med., vol. 37, no. 8, pp. 1513-1521, 2009.
15. P. Narbona, J. Masquijo, F. Barclay, "Anatomia del Ligamento Patelofemoral Medial (LPFM)", Artrosc. (B. Aires), vol. 19, no 3, p. 123-127, 2012. 16. J. McConnell, "Rehabilitation and nonoperative treatment of patellar instability," Sports Med. Arthrosc., vol. 15, no. 2, pp. 95-104, 2007.
17. T. M. Steiner, R. Torga-Spak, and R. A. Teitge, "Medial patellofemoral ligament reconstruction in patients with lateral patellar instability and trochlear dysplasia," Am. J. Sports Med., vol. 34, no. 8, pp. 1254-1261, 2006.
18. M. Ronga, F. Oliva, U. G. Longo, V. Testa, G. Capasso, and N. Maffulli, "Isolated medial patellofemoral ligament reconstruction for recurrent patellar dislocation," Am. J. Sports Med., vol. 37, no. 9, pp. 1735-1742, 2009.
19. J. N. Insall and N. W. Scott, "Clasificación de las alteraciones femororrotulianas," in Rodilla, 3rd ed., vol. 34, no. 3, Madrid: Marbán, 2007, pp. 953-955.
20. E. A. Arendt, D. C. Fithian, and E. Cohen, "Current concepts of lateral patella dislocation.," Clin. Sports Med., vol. 21, no. 3, p. 499, 2002.
21. A. C. Merchant, "Classification of patellofemoral disorders," Arthrosc. J. Arthrosc. Relat. Surg., vol. 4, no. 4, pp. 235-240, 1988.
22. J. P. Fulkerson, "Diagnosis and treatment of patients with patellofemoral pain," Am. J. Sports Med., vol. 30, no. 3, pp. 447-456, 2002.
23. J. P. Fulkerson, "Patellofemoral pain disorders: evaluation and management," J. Am. Acad. Orthop. Surg., vol. 2, no. 2, pp. 124-132, 1994.
24. J. S. Blackburne and T. E. Peel, "A new method of measuring patellar height," J. Bone Jt. Surgery, Br. Vol., vol. 59, no. 2, pp. 241-242, 1977.
25. T. Koshino and K. Sugimoto, "New measurement of patellar height in the knees of children using the epiphyseal line midpoint," J. Pediatr. Orthop., vol. 9, no. 2, pp. 216-218, 1989.
26. J. McConnell, "The management of chondromalacia patellae: a long-term solution," Aust J Physiother, vol. 32, no. 4, pp. 215-223, 1986.
27. Y. Mikashima, M. Kimura, Y. Kobayashi, M. Miyawaki, and T. Tomatsu, "Clinical results of isolated reconstruction of the medial patellofemoral ligament for recurrent dislocation and subluxation of the patella," Acta Orthop. Belg., vol. 72, no. 1, p. 65, 2006.
28. F. Farahmand, W. Sejiavongse, and A. A. Amis, "Quantitative study of the quadriceps muscles and trochlear groove geometry related to instability of the patellofemoral joint," J. Orthop. Res., vol. 16, no. 1, pp. 136-143, 1998.
29. M. Thaunat and P. J. Erasmus, "Recurrent patellar dislocation after medial patellofemoral ligament reconstruction," Knee Surgery, Sport. Traumatol. Arthrosc., vol. 16, no. 1, pp. 40-43, 2008.
30. M. Buchner, B. Baudendistel, D. Sabo, and H. Schmitt, "Acute traumatic primary patellar dislocation: long-term results comparing conservative and surgical treatment," Clin. J. Sport Med., vol. 15, no. 2, p. 62, 2005.
31. E. Nomura, M. Inoue, and M. Kurimura, "Chondral and osteochondral injuries associated with acute patellar dislocation," Arthrosc. J. Arthrosc. Relat. Surg., vol. 19, no. 7, pp. 717-721, 2003.
32. S. E. Christiansen, B. W. Jakobsen, B. Lund, and M. Lind, "Isolated repair of the medial patellofemoral ligament in primary dislocation of the patella: a prospective randomized study," Arthrosc. J. Arthrosc. Relat. Surg., vol. 24, no. 8, pp. 881-887, 2008.
33. P. J. Sillanpää, H. M. Mäenpää, V. M. Mattila, T. Visuri, and H. Pihlajamäki, "Arthroscopic Surgery for Primary Traumatic Patellar Dislocation A Prospective, Nonrandomized Study Comparing Patients Treated With and Without Acute Arthroscopic Stabilization With a Median 7-Year Follow-up," Am. J. Sports Med., vol. 36, no. 12, pp. 2301-2309, 2008.
34. G. L. Camanho, A. de C. Viegas, A. C. Bitar, M. K. Demange, and A. J. Hernandez, "Conservative versus surgical treatment for repair of the medial patellofemoral ligament in acute dislocations of the patella," Arthrosc. J. Arthrosc. Relat. Surg., vol. 25, no. 6, pp. 620-625, 2009.
35. S. M. Desio, R. T. Burks, and K. N. Bachus, "Soft tissue restraints to lateral patellar translation in the human knee," Am. J. Sports Med., vol. 26, no. 1, pp. 59-65, 1998.
36. R. H. Sandmeier, R. T. Burks, K. N. Bachus, and A. Billings, "The effect of reconstruction of the medial patellofemoral ligament on patellar tracking," Am. J. Sports Med., vol. 28, no. 3, pp. 345-349, 2000.
37. P. J. Sillanpää, V. M. Mattila, H. Mäenpää, M. Kiuru, T. Visuri, and H. Pihlajamäki, "Treatment with and without initial stabilizing surgery for primary traumatic patellar dislocationA prospective randomized study," J. Bone Jt. Surg., vol. 91, no. 2, pp. 263-273, 2009.
38. E. Nomura and M. Inoue, "Surgical technique and rationale for medial patellofemoral ligament reconstruction for recurrent patellar dislocation," Arthrosc. J. Arthrosc. Relat. Surg., vol. 19, no. 5, p. 47, 2003.
39. E. T. Ricchetti, S. Mehta, B. J. Sennett, and G. R. Huffman, "Comparison of lateral release versus lateral release with medial soft-tissue realignment for the treatment of recurrent patellar instability: a systematic review," Arthrosc. J. Arthrosc. Relat. Surg., vol. 23, no. 5, pp. 463-468, 2007.
40. R. Clifton, C. Y. Ng, and R. W. Nutton, "What is the role of lateral retinacular release?" J. Bone Jt. Surgery, Br. Vol., vol. 92, no. 1, pp. 1-6, 2010.
41. K. EB., "Factors responsible for the stability of the knee joint.," Bull Hosp Jt. Dis., vol. 18(1): pp. 51-9.
42. C. F. M. Buckens and D. B. F. Saris, "Reconstruction of the Medial Patellofemoral Ligament for Treatment of Patellofemoral Instability A Systematic Review," Am. J. Sports Med., vol. 38, no. 1, pp. 181-188, 2010.
43. P. Schöttle, A. Schmeling, J. Romero, and A. Weiler, "Anatomical reconstruction of the medial patellofemoral ligament using a free gracilis autograft," Arch. Orthop. Trauma Surg., vol. 129, no. 3, pp. 305-309, 2009.
44. K. R. Reddy and N. S. Reddy, "Trochleoplasty and medial patellofemoral ligament reconstruction for recurrent patellar dislocation," Indian J. Orthop., vol. 46, no. 2, p. 242, 2012.
45. P. B. Schöttle, A. Schmeling, N. Rosenstiel, and A. Weiler, "Radiographic landmarks for femoral tunnel placement in medial patellofemoral ligament reconstruction," Am. J. Sports Med., vol. 35, no. 5, pp. 801-804, 2007
